Hear why graduate students chose SUNY Cortland
Ashley Antoine
Minju Oh
Classroom Experiences
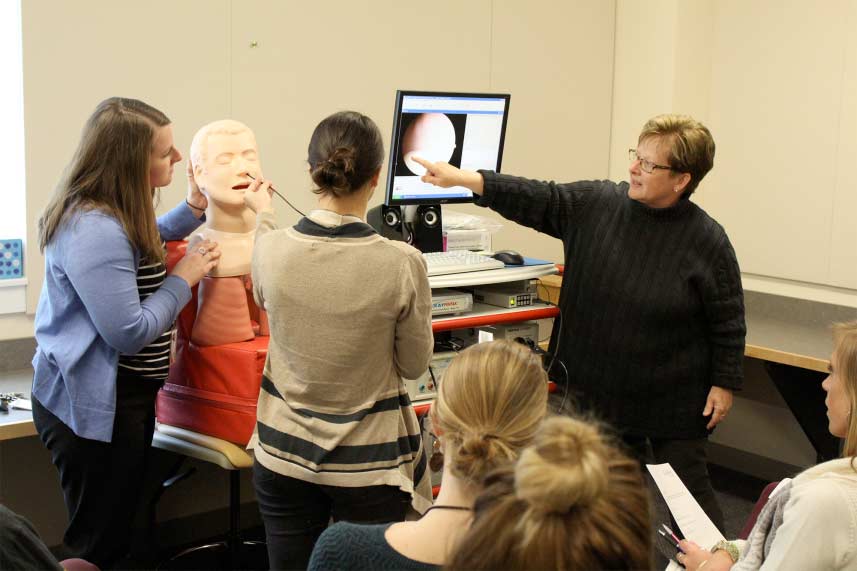
Instrumentation
Using an endoscope and a mannequin that they nicknamed Seymour Bolus, students learn about flexible nasoendoscopy. Read more about their hands-on practice in the classroom.
Students practice using an Electrolarynx, a battery-powered device that generates a sound using vibrations, to understand how individuals might communicate after undergoing a total laryngectomy for head and neck cancer.

Augmentative and Alternative Communication
Graduate students learn about Augmentative and Alternative Communication (AAC) technology like eye gaze technology, a device that allows people to control a computer or tablet by looking at words or prompts on the screen. See a graduate student using scanning with electromyography to make choices on an AAC device.

Communication Disorders in Adults
June is National Aphasia Awareness Month. During a summer course, students led educational sessions in the community on a communication disorder that results from damage to the parts of the brain containing language. Students also created and distributed “aphasia-friendly” menus to local restaurants and assisted living facilities.
Read more about their work to raise awareness on this language disorder.

Dysphagia
Students, faculty and staff members participated in the thickened liquid challenge to increase awareness of dysphagia, which is commonly associated with difficulty swallowing.

Assistive Technology
Graduate students had an opportunity to try out Obi, an adaptive eating device for individuals with upper extremity strength and mobility limitations. This device was brought in from an assistive technology lending library, Technology Related Assistance for Individuals with Disability (TRAID), in New York.